By Joanne Lynn and Sarah Slocum
“All models are wrong, but some are useful”. – George Box
In late November, the Centers for Medicare and Medicaid Services (CMS) released an extensive evaluation of the Community-based Care Transitions Program (CCTP). (https://downloads.cms.gov/files/cmmi/cctp-final-eval-rpt.pdf)
While the report has some useful points, the primary metrics used to measure performance – re-hospitalization/discharge rates, are seriously deficient. To start with, reducing hospital readmissions – or, for that matter, reducing admissions – is not always good for patients. More importantly, the CCTP evaluation presumed that the relevant part of the patient’s journey starts in the hospital at discharge, and that the main issues revolve around having and adhering to the correct discharge instructions, especially for medications, which then lead to engaging the patient in his or her outpatient medical care. These are certainly important, but the evaluation’s narrow focus on short-term transitions of care leaves out much of what happens in the lives of seriously ill persons that reflect the capacity of their community to provide ongoing supportive services – disability-adapted housing, home-delivered nutritional food, the adequacy of the personal care workforce, employer flexibility for family caregiving, and more.
The CCTP was part of a larger innovation effort sponsored by CMS, the Partnership for Patients, which had an overall goal of a 20% reduction in Medicare fee-for-service (FFS) hospital readmission rates. The agency was given $500 million to implement CCTP in 101 sites around the country. Most project sites applied basic commonsense transitions of care protocols, for which there is substantial evidence, i.e., ensuring that newly discharged patients received the right medications and were engaged with their community-based physicians in order to prevent avoidable hospital readmissions within 30 days after discharge. Yet the focus on medical services provided at and for a short while following hospital discharge, as well as the metric that applied to hospital rates, distorted the endeavor and put a good number of participating community-based organizations at serious financial risk.
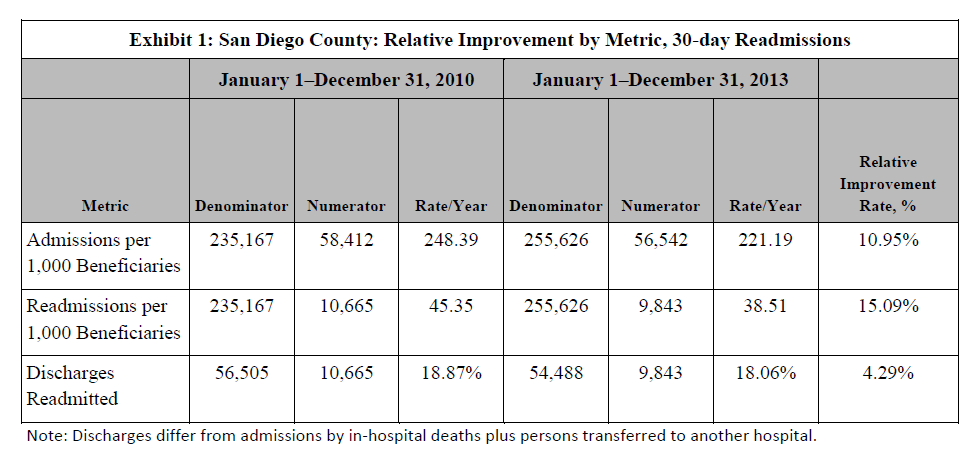
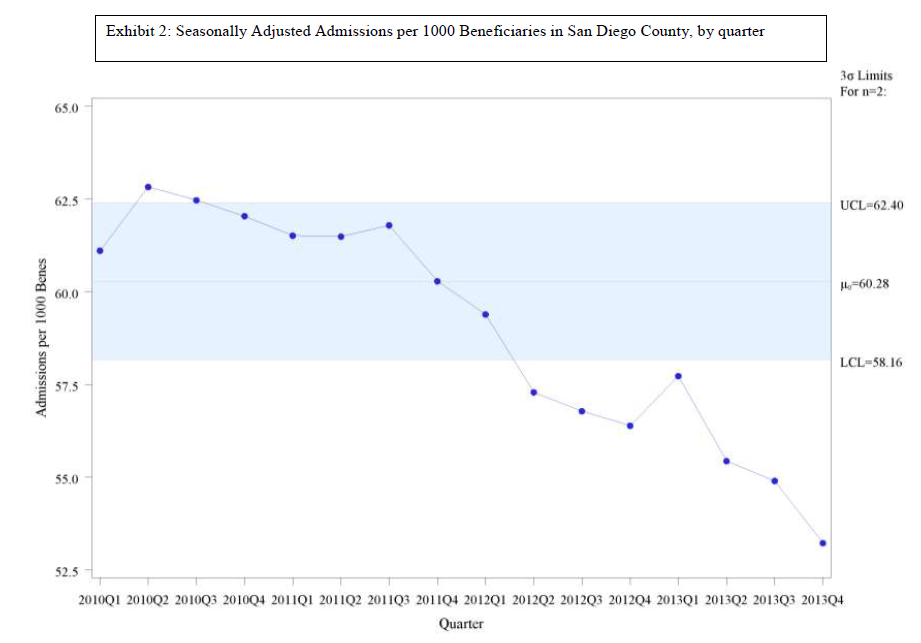
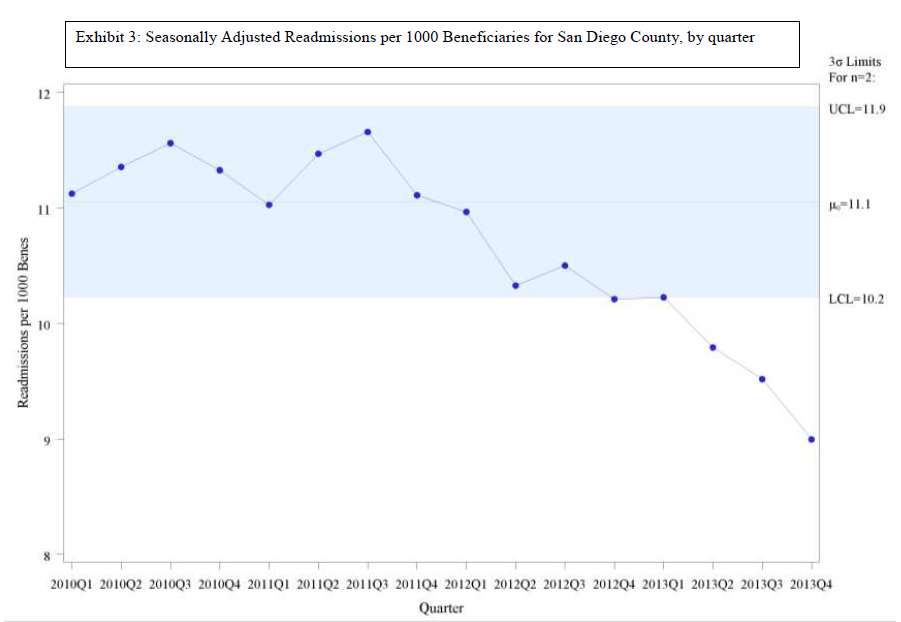
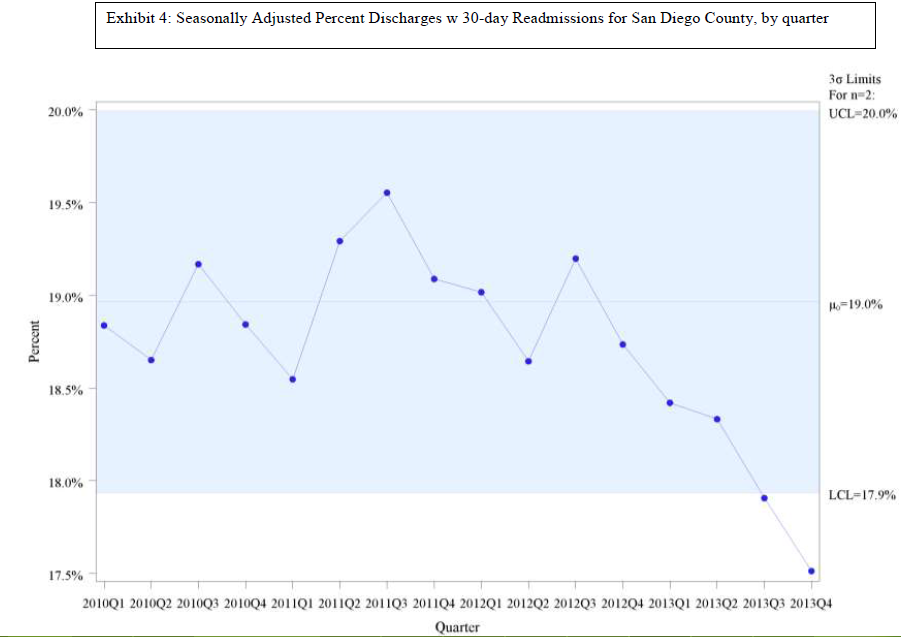
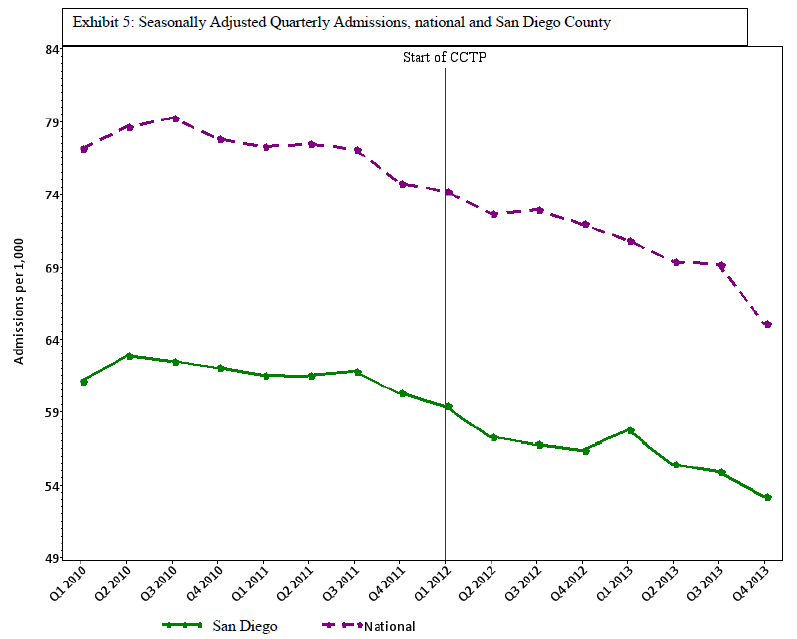
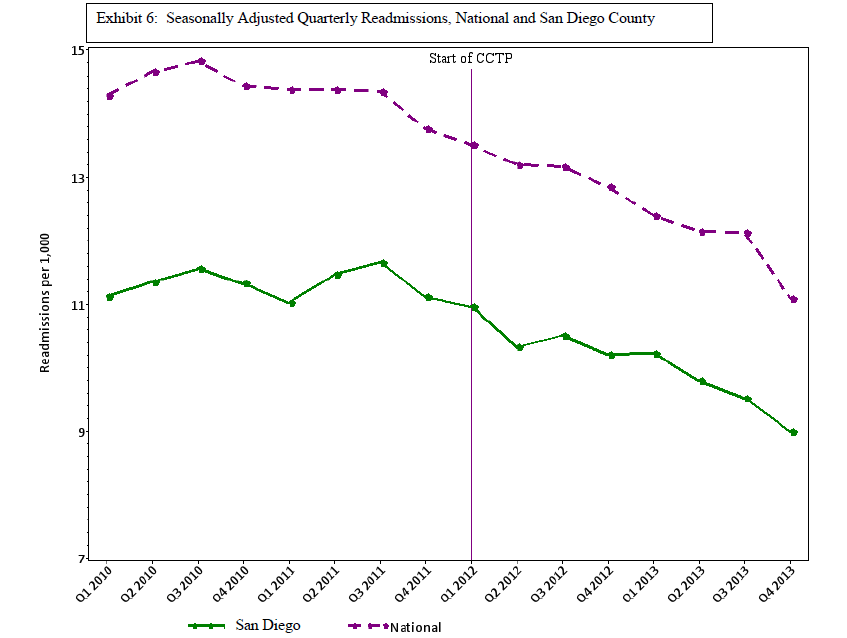
The original Quality Improvement Organization (QIO) project that preceded the CCTP measured the effect of improvement activities on entire communities (rather than specific hospitals), and aimed to reduce readmissions per 1,000 Medicare FFS beneficiaries across the entire population, https://jamanetwork.com/journals/jama/fullarticle/1558278. That model accepted the need not only to address medical errors and mobilize patient self-care, but also to focus on what it takes to successfully shift the support of very sick and disabled persons to community service providers and reduce the challenges of living with ongoing serious illness.
In the QIO project, most Medicare beneficiaries who were re-hospitalized within 30 days were known to be very sick and disabled prior to the initial hospitalization. This meant that the hospitalization episode represented a few somewhat worse days in the course of living with a serious condition, such as an organ system failure, neuromuscular degenerative disease, or frailty. That understanding broadened the focus of reforms to include examining the capacity of the person’s community to support very sick and disabled persons with reliability and competence. The interventions aimed to optimize the overall course of disease and disability and to ensure that the individual and family (and other caregivers) felt well supported. For example, they worked to ensure the adequacy of the care plan, prompt availability of supportive and personal care services, and realistic planning for decline and death.
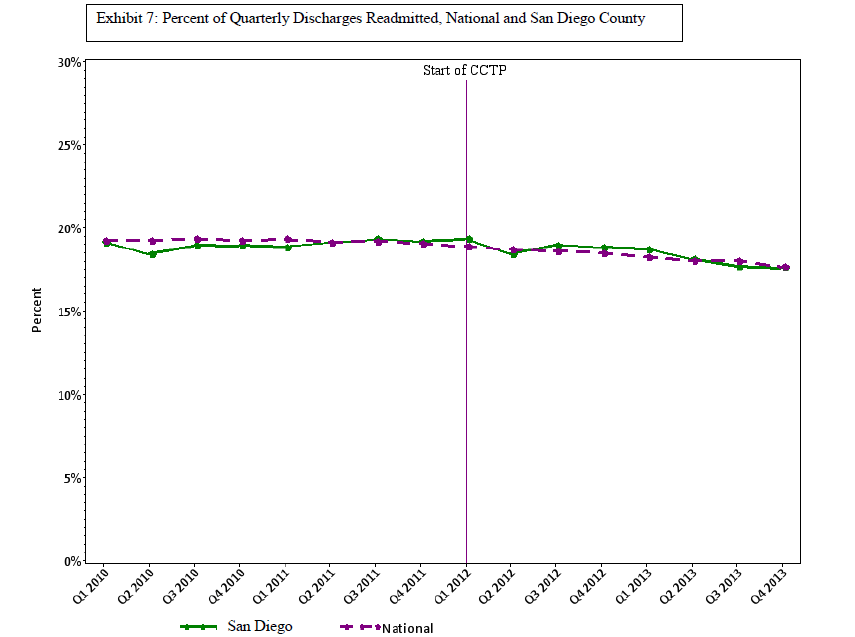
However, in building on the QIO results, CMS shifted the focus to a hospital-centric design and evaluated performance on a hospital-specific basis. This creates the problem that we reported in a previous blog, https://medicaring.org/2014/12/08/lynn-evidence/, which is that good practices in the community reduce the number of admissions at about the same rate as the number of readmissions, is ignored. In turn, this makes the hospital-based readmissions/admissions metric misleading. Perhaps more important, structuring the CCTP to measure the impact only on the hospital leaves out the importance of how effective community-based providers were in providing supportive services over time to frail elders living at home and in other community settings.
Some community services providers nevertheless managed to help their partnering hospitals make impressive gains in reducing re-admissions. For example, the Eastern Virginia Care Transitions Program (EVCTP) brought together five Area Agencies on Aging that improved support and smoothed transitions across 20% of the state. Five health systems and 69 skilled nursing facilities joined. Re-hospitalizations for the whole area declined from 18.2% of all FFS Medicare discharges in 2013 to 8.9% in 2015, resulting in a $17 million savings to Medicare and a great deal of avoided suffering by patients, families, and caregivers. EVCTP used the Coleman Care Transitions Intervention© and offered enhanced services as part of the admissions process for certain segments of the Medicare population. It also prompted formation of a coalition of all 25 Area Agencies on Aging in Virginia to infuse best practices in subsequent partnerships across the state, http://www.chcs.org/media/EVCTP-Case-Study_101217.pdf/.
In Akron, Ohio, “Direction Home,” the Area Agency on Aging’s program, first began embedding coaches (either nurses or social workers) in local hospitals in 1998 to assist patients through connecting them to various community services, including home care and home delivered meals. That history of collaboration between health care providers and social services providers gave Akron a head start in reducing hospital use by Medicare beneficiaries with ongoing serious chronic conditions. Between 2010 and 2016, hospital readmissions fell from 19.6% of Medicare FFS hospital discharges to 11.7%. Akron leaders attribute much of this success to intentional relationship building, which extends to having health system professionals on the boards of community organizations, http://www.commonwealthfund.org/publications/case-studies/2017/aug/akron-ohio-health-care. However, CMS did not allow community-based organizations to use CCTP funds for training, overhead, data development, administration, or outreach – only for the patient-facing services. This meant that some of the community-based organizations encountered major difficulties and high costs in trying to forge initial connections and close working relationships with hospitals in their area.
Other findings in the evaluation point to well-documented challenges for some CCTP sites, including incorrect (or poorly understood) discharge instructions on medications and dietary restrictions; under-resourced community-based services; fragmentation between social services and health care systems; and a lack of data at the individual level for high-value individual care planning, and at the aggregate level for geographically-based system planning.
Every model leaves out a great deal of complexity. What matters is what we retain and take forward in subsequent work. We can accept that high re-hospitalization rates are probably evidence of shortcomings in a hospital’s discharge processes, and that mobilization of patients to take care of themselves gets us partway toward a better model of care. However, we should also include how communities and their social support organizations can improve access to adequate safe housing, nutritious food, reliable personal care, and other key services. That more complex model requires the involvement of multiple stakeholders, and measuring the performance of a complex, multi-faceted care system that serves similarly situated individuals across a geographic community — rather than just the re-hospitalization rates of certain hospitals.